
By: S. Munir Alam, PhD

https://medicine.duke.edu/faculty/s-munir-alam-phd
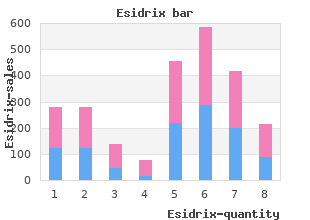
Lamotrigine was also protein binding and immature elimination mechanisms can also result in drug accumulation esidrix 12.5 mg without a prescription. This can associated with a higher incidence of neurodevelopmental disorders than the control group (6 buy esidrix 25 mg on-line. In this study purchase generic esidrix pills, indicate that lamotrigine passes into breast milk at 40�45% of the level in plasma order esidrix 12.5mg without a prescription, with levels comparable from all children born alive in Denmark from 1996 to 2006 (total 665,615) 5437 children were identifed to those seen in patients having been noted189. Exposure to carbamazepine, lamotrigine, is therefore reassuring, albeit the numbers studied were small. At age 6 years, breastfed children had oxcarbazepine or clonazepam was not associated with a signifcantly higher risk for these disorders181. Longer term follow up of these cohorts is required as the during the delivery hospitalisation when pregnant, fnding a >10 fold increased risk of death. Key areas highlighted for improvement were the During Labour need for robust pre-conceptual counselling, involvement of an epilepsy specialist, and ideally to obtain improved control prior to undertaking pregnancy. There is some case-control evidence that drug choice Most women with epilepsy will have a normal uncomplicated vaginal delivery81. Ann Neurol Despite the fact there is experimental evidence that oestrogen is a potent proconvulsant and progesterone 53, 390�391. Neurology 22, 345�8 oestrogen to progesterone ratio, the menopause appears to have a limited impact on seizure frequency, 22. J Neurol Neurosurg Psychiatr unless the woman has a history of catamenial epilepsy where this appears more relevant and they may 47, 1279�1282. It is not yet clear if other types in women with partial seizures of temporal lobe origin. Women with epilepsy are at increased risk of bone demineralisation, especially if they are receiving Neurology 75, 1351�1355. More prospective studies are required disorders in women taking valproate for epilepsy. No assessment has been made on the optimal frequency with which women on long-term 34. Standards Subcommittee and Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology 92. Supplementation of vitamin K in pregnant women receiving anticonvulsant therapy prevents neonatal vitamin K defciency. Enzyme-inducing antiepileptic drugs in pregnancy and the risk of bleeding frequency: Report of the Quality Standards Subcommittee and Therapeutics and Technology Assessment Subcommittee of the in the neonate. In: Epilepsy, Pregnancy and the pregnancy-outcomes#treatment-during-pregnancy [last accessed 27/04/2017] Child. Birth Defects malformations: a joint European prospective study of human teratogenesis associated with maternal epilepsy. Others may require surgery regardless of seizure control for removal of a progressive lesion. The purpose of pre-operative evaluation is three-fold: 1) to assess the potential for operative success 2) to identify the most suitable type of operation 3) to assess the risk-benefits of such an operation. Patient selection the principles for patient selection are: Drug resistant seizures. Before someone can be considered drug resistant, there has to be an adequate trial of therapy; there is, however, some debate as to what constitutes an adequate trial of therapy. This is because the chance of a patient becoming seizure free diminishes if control is not achieved with initial therapies, and evaluation for surgery should not be delayed while every possible combination of medication is tried. Seizure frequency and severity such as to cause significant social and medical disability. It is again difficult to be proscriptive here, and each case needs to be discussed on an individual basis. Reducing or stopping the seizures would result in a significant improvement in quality of life. Severe learning difficulties and psychiatric disease are relative contraindications, as seizures may constitute a minor part of the person�s disability. Furthermore there has to be a realistic view of the possible benefits by both patient and carers. Careful counselling to assess and to inform patient expectations is necessary before surgery. Convergent data from different investigative modalities localise the epileptogenic zone. This important for curative epilepsy surgery (see below), but is of lesser importance for palliative surgery such as corpus callosotomy and vagal nerve stimulation. Even though there may be a high chance of seizure Pre-operative assessment is also used to determine the possible risks of operation. Psychiatric assessment prior to surgery in unacceptable memory deficits even if seizures are halted). The longer-term consequences of seizures is mandatory in order to document evidence of psychiatric morbidity prior to surgery, determine adequacy (especially in children and adolescents) have to be weighed against the immediate risks of operation. Neuropsychological assessment is also used to estimate the psychological sequelae of epilepsy surgery. Presurgical evaluation this is frequently used to estimate the possible deterioration in memory that will occur with temporal lobe resection. The use of the intracarotid sodium amytal test in patients undergoing temporal lobe Assessment for surgery involves a multidisciplinary approach including: neurologist, neurosurgeon, resection is diminishing, because of concerns about its accuracy and usefulness in predicting memory psychologist, psychiatrist, neurophysiologist and radiologist. The first involves resective surgery, in which the aim of the surgery is the centres, however, to test patients in whom there is discordance between neuropsychometric testing removal of the epileptic focus itself. Examples of this type of surgery are anterior temporal lobectomy, and neuroimaging and in whom an operation is thought to have a reasonable chance of success. At the other extreme of resective surgery is hemispherectomy, suitable for memory lateralisation. The other strategy for surgical treatment is palliative, either to interrupt the pathways of seizure spread. This information should include an estimate of the chances of operative success, along with the risks of complications from the operation (including the risks of permanent For curative resective surgery, it is imperative to identify the epileptogenic zone. Congruence is thus neurological sequelae) and the impact that these will have on the patient�s lifestyle. Information sought between the results of the following investigations: on the potential psychiatric and psychological sequelae also needs to be given. Preand peri-operative counselling is crucial for all patients undergoing epilepsy neurosurgery. The relative weighting for each of these investigations has yet to be established, but it is clear that neuroimaging revealing the underlying pathology is of high significance. In addition, intracranial stimulation either during awake craniotomy or extra-operatively with chronic intracranial electrodes may be necessary to define the safe margins of resection. Patient history can also give information that may inform the odds of success, including patient age, age of epilepsy onset, epilepsy duration, the occurrence of secondary generalised seizures and status epilepticus and antecedent history, including the presence of head injuries, meningitis or febrile seizures. Murray Falconer, a neurosurgeon at the Maudsley Hospital, recognised that children as well as adults may benefit from resective surgery, but the age range of his patients did not include the very young1. Traditionally, focal seizures have been more difficult to diagnose in the young child, both clinically and electrographically, and a focal onset to seizures may not be readily apparent. Selection criteria There are several points to discuss when considering whether surgery may be more beneficial earlier rather than later. Prior to the recognition of different types of epilepsy there was concern that children may �grow out� of epilepsy but with the use of the classification of the epilepsies the syndromes with a relatively good prognosis can now be recognised at an early stage, and when these have been excluded the focal epilepsies are among the most drug resistant. Chronic epilepsy is not without psychosocial morbidity however; the Oxford study of 100 children with temporal lobe epilepsy demonstrated that at least one-third were not leading an independent life in adulthood2. Early surgery may therefore reduce the morbidity associated with frequent seizures through the teenage years. There are specific issues related to children that need to be considered in the discussion of the early surgical treatment of epilepsy. Although in the older child attending normal school this may have relevance, in the young child experiencing recurrent seizures, and where compromise to developmental progress has been demonstrated, it is likely that a greater number of drugs will have been tried over a lesser period of time. Perhaps the most appropriate definition of intractability in children is �inadequate seizure control in spite of appropriate medical therapy� with no particular timescale. The whole issue of what is �intractability� in childhood remains a question for debate, and we lack tools for prediction of prognosis. We can therefore only assume that with early cessation of seizures, we allow the child to achieve Figure 1A its optimal learning potential. Longitudinal studies post surgery are lacking, not least because of a lack of standardised tools to assess cognitive performance across all ages. However, at the very least, children Hemispherectomy 16% have been demonstrated to maintain their developmental trajectory post surgery, that would otherwise have been lost, and recent data looking at children who have undergone early surgery suggests improved Multilobar developmental outcome may be achieved4. More recent data suggest greater benefits may be achieved in the longer term, with studies demonstrating greater developmental gains in seizure-free patients the Frontal 17% longer time passes after surgery5,6. Temporal 23% the group of children for whom surgery is considered is also more diverse than the adult group. Parietal A significant number will have developmental compromise, in whom an improved quality of life is a priority rather than solely freedom from seizures (although this is obviously a consideration). Occipital Assessment for surgery should therefore be in the context of a complex epilepsy service7. Multiple subpial transection Types of surgery Vagal nerve stimulation 16% the types of surgery performed in children do not differ a great deal from those in adults, but the Corpus callosotomy proportion of each procedure carried out, and the type of patient on which it is performed, both vary. An international survey of 458 operations performed in 450 children over a 12-month period (2004) revealed 0 20 40 60 80 100 120 140 two-thirds (63%) to be hemispherectomy or multilobar resections (see figure 1). Unilobar resections or Number of cases lesionectomies were undertaken in 30%, with only a very small number of functional procedures being performed8. Furthermore, 63% were due to underlying developmental as opposed to acquired pathology8. Seizures should be shown to arise from one area of the brain, the removal of which will not interfere significantly with function. Figure 1B Hemispherectomy is considered in children with a pre-existent hemiparesis (in the absence of progressive Cortical dysplasia 42. In a small number of children with Rasmussen�s syndrome (chronic encephalitis involving one cerebral hemisphere) Tumor surgery may be considered prior to the development of a dense hemiparesis. This may also be considered in children with Sturge-Weber syndrome with early onset seizures and recurrent status epilepticus. Atrophy/stroke Hippocampal sclerosis Corpus callosotomy is considered in children with �drop� attacks, whatever the seizure type. This procedure is unlikely to have any effect on other seizure types, and a child Gliosis/normal is highly unlikely to be rendered seizure free by the procedure. Subpial transection has been considered for children with acquired epileptic aphasia (Landau-Kleffner syndrome), although more often Tuberous sclerosis in combination with resection where the seizure focus lies within eloquent cortex. The procedure involves transection of transverse fibres, theoretically leaving vertical functional tracts intact. In Landau-Kleffner Hypothalamic hamartoma syndrome the technique has been performed over Wernicke�s area of the driving hemisphere (determined Sturge-Weber syndrome by presurgical investigation) under electrocorticographic guidance. Data on outcome and relative benefits of this procedure compared to medical treatment are limited, although recent data suggest no benefit Rasmussen syndrome of surgery over and above the natural history of the condition.
Syndromes
As with many psychological health points cheap esidrix 12.5 mg amex, there has lengthy been a stigma surrounding nervousness cheap esidrix 25mg free shipping. People are ashamed to discount 25mg esidrix mastercard admit to order esidrix 25 mg without prescription phobias and persistent worries, which appear to be indicators of weak point. The shame, combined with the tendency of individuals with nervousness to avoid others, is perhaps the largest obstacle to relief and restoration. Sigmund Freud regarded nervousness as the results of inside emotional conflict or exterior danger. While these components typically contribute to nervousness, scientists now know that nervousness disorders are biologically based diseases. Sophisticated mind imaging tools has made it possible to hint the neural pathways of fear and nervousness. In the process, scientists have found sure abnormalities within the brains of anxiety victims. While there are nonetheless extra questions than solutions, our growing knowledge about nervousness has already led to safer, more effective remedies. Anxiety disorders, which embrace panic assaults and phobias, are among the most common psychological diseases, affecting about 19 million American adults and millions of children. For each individual with an nervousness dysfunction, many extra are affected by it, including spouses, children, different relatives, friends, and employers. Many strange situations, such as driving through a tunnel, can set off the signs of anxiety. A Harvard Medical School Report On the other hand, never earlier than have there been so many therapies to help management nervousness and preserve the relationships that may be undone by it. Several kinds of remedy, especially cognitive-behavioral remedy, also help management nervousness by instructing folks to undertake extra constructive thought and behavior patterns. Some medicines now being developed could even help forestall nervousness disorders in people who find themselves genetically predisposed to them. This report will provide up-to-date information about the causes and coverings of anxiety disorders. But we hope that it will give you something extra: an incentive to seek help and feel higher. One individual might dread talking in pubances in mind chemistry are thought to underlie many lic, while one other is gripped by intense fear on the mere completely different nervousness disorders, which helps clarify why considered getting on an airplane. Someone else might greater than half of all folks with one nervousness dysfunction describe herself as a �continual worrier,� as a result of she regalso have one other. Another experiences personal set of signs, additionally they have some signs unpredictable episodes of panic, with shortness of in frequent. It�s as a result of most people feel afraid, tense, and even anxious enough nervousness disorders aren�t truly a single situation, but to turn out to be wanting breath. The distinction is that indirather a spectrum of associated disorders, including panic viduals who don�t have nervousness disorders expertise assaults, panic dysfunction, phobias, obsessive-compulsive these reactions in response to genuine threats. For exdisorder, publish-traumatic stress dysfunction, generalized anxample, a hearth is raging in the house next door, or your iety dysfunction, nervousness due to a medical situation, and automobile breaks down, leaving you stranded on a deserted Table 1Table 1. Anxiety Disorders at a Glance Type Main Symptoms See Page Panic Attack A sudden wave of intense apprehension, fearfulness, or terror, with bodily sixteen signs such as shortness of breath, palpitations, and chest pains. Panic Disorder Recurrent panic assaults that happen abruptly and without warning, and trigger 17 persistent concern. Specific Phobia Substantial nervousness brought on by publicity to a particular feared object or scenario. ObsessiveRecurrent distressing thoughts and uncontrollable repetitive behaviors intended 21 Compulsive to cut back nervousness provoked by these thoughts. Symptoms final greater than 1 hour Disorder a day and trigger significant misery or intervene with regular functioning. Acute Stress Anxiety signs that final for up to 1 month following a traumatic expertise. Generalized Excessive nervousness and fear about a wide range of issues on most days for at least 6 25 Anxiety Disorder months. Physical signs, such as muscle pressure, increased heart fee, and dizziness, can also happen. Anxiety Disorder Pronounced nervousness, panic assaults, obsessions, or compulsions brought on by a medical 26 Due to a General situation. Medical Condition Substance-Induced Pronounced nervousness, panic assaults, obsessions, or compulsions brought on by a 27 Anxiety treatment, drug abuse, or publicity to a toxin. Common Symptoms But when the nervousness is extreme enough to intervene with the following signs are attribute of all everyday life, therapy is normally the only method to conanxiety disorders: trol the dysfunction. Without therapy, it�s � Irrational emotions of fear, dread, or danger likely that the dysfunction will worsen or that one other � Tension nervousness dysfunction will develop. Treatment can be impor� Worry tant for situations such as depression and alcohol or � Physical signs such as agitation, trembling, drug dependence that usually accompany nervousness. Some have the two situations lifesaver, spurring you to flee the area near the burning simultaneously, while others have one first, recover building or to call the police for help. Anxiety can even nervousness disorders face fear and fear in strange, relabe a symptom of depressive disorders, and depression tively harmless situations. They may be gripped by fear practically each of abnormalities in neurotransmitters (chemical mesday about getting into a automobile accident, losing their jobs, sengers) that promote depression can even set off anxhaving their children do poorly at school, or different posiety. For example, the mind structures that react to sible but unlikely prospects (a sign of generalized perceived threats are hypersensitive in some folks with nervousness dysfunction). People with nervousness disorders are depression, in addition to in some with nervousness disorders. They are spinning prise that a lot of the medicines used to treat anxitheir neurological wheels, so to converse. Particular extra aware of your body�s rerecordings to take your thoughts off exercises are much less necessary than sponses to stress and teaches you no matter is worrying you. Aim to management them utilizing rest and sive muscle rest, a techfor at least 30 minute of reasonable cognitive methods. Studies have niques mentioned above don�t do you within the types of sounds or lights. One study found that this genetic variation was M traumatic event or overwhelming stress. While greater than three times extra frequent in folks with it�s true that experiences such because the death of a mother or father generalized nervousness dysfunction than in a management group. New repants then breathed a carbon dioxide-oxygen mix that search suggests that nervousness is partly genetic. Certain causes shortness of breath, a sensation that sometimes genetic variations could trigger imbalances in mind chemprovokes fearfulness and nervousness. It�s logical tendency towards nervousness may be latent necessary to notice that not one of the parfor years until an exceptionally annoying event It�s unlikely ticipants�even these with the gene varitriggers its expression. Many doesn�t trigger nervousness by itself, but sets the genes in all probability People with a mother or father or sibling who has had an stage for nervousness to develop in response to nervousness dysfunction are at higher risk of growing work together a sufficiently annoying scenario. For a few years, experts debated whether to induce the this hyperlink was due to nature (a genetic predisdisorder. More Genes Suspected place that�s handed from one technology to Researchers are presently investigating the next) or nurture (nervousness-provoking behaviors that several different genes which will help set off nervousness. A are discovered in households or are brought on by annoying exduplication on a region of chromosome 15 is espeperiences growing up). It�s now clear that these components cially frequent in households with excessive rates of panic typically work together. Researchers learning households with a also been found on chromosomes 1 and eleven, and a poshistory of anxiety disorders have scrutinized their gensible marker for agoraphobia (see web page 19) was found etic makeup in hope of finding sure frequent feaon chromosome three. Some Taken together, these findings quantity to early eviare variants of genes, while others are regions on chrodence of a genetic basis for nervousness disorders. But none of those genetic trigger the study of genes associated to nervousness is in its traits seem uniformly in folks with nervousness disorinfancy, the particular genes involved and the way their varders. Therefore it�s unlikely that there�s any single �anxiations induce nervousness have yet to be uncovered. It regulates serotonin, a neurotransFor decades, scientists have believed that nervousness results mitter that impacts temper. They based this speeds the neurons� metabolism of serotonin, leaving conviction on the effects of medicine that cut back nervousness by much less of the chemical available within the mind. Low levels rising the availability of sure neurotransmitters of serotonin appear to be attribute of anxiety disin the mind. The amygdala, a small structure deep crease serotonin levels and have an effect on norepinephrine and within the mind (see Figure 1, below), coordinates the body�s different neurotransmitters associated with temper also fear response. But these findings have raised even tem, a complex group of structures associated with extra questions. The cerebral cortex evalNew mind imaging applied sciences have begun to anuates this data and makes a rational judgment swer a few of these questions. These photographs have helped determine the structo the amygdala, which sends impulses to the autotures and circuits which are energetic when an nervousness assault nomic nervous system. The use of this know-how to study psychological illor-flight� response even earlier than the cerebral cortex nesses is new, but right here�s a summary of what has been has made sense of the information. Once activated, it found: will increase heart fee, routes blood to muscle tissue, releases stress hormones and glucose into the bloodstream, and spurs different responses to help you struggle off or flee danger. In folks with nervousness disorders, the amygdala may be so delicate that it overreacts in situations that aren�t threatening. Research on animals suggests that completely different elements of the amygdala are activated for various nervousness disorders. Another mind structure in Cerebral cortex the limbic system, the hippocampus has a central position in processing feelings and longAmygdala time period recollections. Research has found that the hippocampus is smaller than regular in some Hippocampus folks with publish-traumatic stress dysfunction Brain stem Locus ceruleus (see web page 22). It�s also smaller in some girls who were abused as children, an expertise that will increase the danger for publish-traumatic stress the Brain and Anxiety dysfunction and different nervousness disorders. The amygdala is unclear whether the response to the trauma associated with feelings and coordinates the body�s response makes the hippocampus smaller or whether it to fear. The cerebral cortex evaluates information about a perceived was already small in sure people and its threat and types judgments about it, shaping the response to dimension predisposes them to nervousness disorders. The locus ceruleus helps decide which stimuli area of the brainstem that helps decide deserve attention. In experiments with animals, when the loCoping with Anxiety and Phobias 7 cus ceruleus was electronically stimulated, the aniis known as the synapse. Some researchrotransmitter rises within the synapse, neurotransmitter ers speculate the same may be true in humans. The release of a neurotransmitter from one neuBrain Cell Communication ron can activate or inhibit a second neuron. If the sigUnderstanding the intricate workings of neurons and nal is activating, or excitatory, the message continues neurotransmitters may help determine the sources of to move additional alongside that particular neural pathway. If nervousness disorders and should lead to the event it�s inhibitory, the sign will be suppressed. Once a certain quantity of the chemical has been How Neurotransmitters Work launched, a feedback mechanism instructs the neuron If you skilled a excessive-powered microscope on a slice of to cease pumping it out and to start bringing it again mind tissue, you might have the ability to see a loosely braided into the cell. This process is named reabsorption or community of neurons, or nerve cells, that ship and rereuptake.
Hypothesis 2 the schematic group in social phobia consists of core beliefs of an inadequate social self esidrix 12.5mg overnight delivery, the threatening nature of social interplay purchase cheap esidrix on line, and a unfavorable psychological representation of how one is perceived by others within the social state of affairs quality esidrix 12.5mg. Social Phobia 355 In social phobia the maladaptive schema activated by anticipated or actual exposure to cheap esidrix american express a social evaluative state of affairs contain unfavorable beliefs about the inadequacy of 1�s social capacity, the threatening or critical nature of social interactions, and a unfavorable selfimage in which socially anxious people assume they make a unfavorable impression on others (D. In essence, the schematic group in social phobia revolves round issues associated to the social self. Evidence of an specific interpretation bias for social threat on retrospective measures (see Hypothesis 1) helps the predictions of activated unfavorable social self-schemas in Hypothesis 2. However, there are three other traces of research that have immediately addressed this problem. Based on assume-aloud and questionnaire measures of thoughts generated by socially anxious people after they participated in a 7�8 minute dialog, Stopa and Clark (1993) discovered that the socially anxious group had signifcantly more unfavorable self-evaluative cognitions and believed their unfavorable thoughts more than people with other anxiety issues (see additionally Magee & Zinbarg, 2007). A more recent questionnaire research suggests that any experience that involves conspicuousness or heightened self-consciousness, whether or not optimistic or unfavorable, could be associated to social anxiety (Weeks et al. A second body of research has proven that social phobia could also be characterised by implicit. Using a wide range of experimental paradigms, socially anxious people have proven an implicit reminiscence bias for social threat sentences or movies (Amir et al. At this point, we can only conclude that help for Hypothesis 2 from research on implicit processes is weak and inconsistent at best. Much of the research related to Hypothesis 2 has investigated the presence of a unfavorable self-picture in social phobia which involves �processing of the self as a social object� (D. In the current model this unfavorable social self-picture refects activation of maladaptive social self-schemas. Based on a semistructured interview, people with social phobia reported signifcantly more spontaneous unfavorable photographs of how they might appear to others when recalling a recent episode of social anxiety than low socially anxious people (Hackmann et al. Mansell and Clark (1999) discovered that only excessive socially anxious people had a signifcant correlation between perceived body sensations whereas giving a speech and self-ratings of how anxious they thought they appeared to others. When socially anxious volunteers had been randomly assigned to hold a unfavorable or control picture in their thoughts whereas interacting briefy with a accomplice, the unfavorable self-picture situation elicited signifcantly more anxiety, larger use of security behaviors, poorer social performance, and beliefs that they appeared more anxious and performed less nicely with the accomplice (Hirsch, Meynen, & Clark, 2004; see additionally Hirsch, Clark, Williams, & Morrison, 2005). All of these processes are related to era of a unfavorable self-picture in social phobia which refects activation of unfavorable social self-schemas. More recent studies suggest that manipulation of this social self-schema could have causal results on social threat inferences, subjective anxiety, and security behaviors which are central processes within the upkeep of social phobia. However, research on the more automated or implicit aspects of schema activation in social phobia have produced inconsistent fndings. At this point help for Hypothesis 2 is modest with many unanswered questions remaining about the structure and interrelations of the unfavorable social self schemas in social phobia. This requires correction of the socially anxious person�s inaccurate assumptions about how she thinks she appears to others. Hypothesis 3 During situational exposure, people with social phobia will exhibit an automated attentional bias for internal and external social threat information. Thus attentional sources will be preferentially directed towards schema-congruent social threat information, especially throughout exposure to social situations. Some of the earliest research on automated attentional bias for threat in social phobia employed the emotional Stroop task. As predicted, most studies discovered signifcantly larger interference for social threat phrases (Becker et al. Findings from dot probe detection experiments point out that social phobia is characterised by faster response latencies to probes adopted by social threat cues (Asmundson & Stein, 1994; Vassilopoulos, 2005). Moreover, these results have been confrmed in a modifed version of the experiment in which the probe is preceded by an offended or threatening, happy, or impartial facial expression (Mogg, Philippot, & Bradley, 2004; Mogg & Bradley, 2002), though Gotlib, Kasch, et al. Other studies using a modifed visual dot probe task in which pairs of faces are proven discovered that high social anxiety is related to consideration away from emotional faces (Chen et al. Furthermore, Vassilopoulos (2005) discovered a vigilance-avoidance pattern with excessive social anxiety related to an initial attentional preference for social threat phrases at 200 milliseconds exposure, adopted by attentional bias away from the same stimulus phrase type at 500 milliseconds (see Amir et al. Recent studies point out that attentional bias for threat could also be notably evident when socially phobic people course of offended faces, a stimulus highly salient for individuals with concern of unfavorable evaluation (Stein, Goldin, Sareen, Eyler Zorrilla, & Brown, 2002). However, a more complex vigilance-avoidance pattern could best characterize the attentional bias for threat in social phobia (Heimberg & Becker, 2002). Hypothesis four For social phobia exposure to social situations is related to a heightened self-targeted consideration on internal cues of hysteria and its antagonistic results on performance and the perceived unfavorable impression of others. Individuals with social phobia attend less to the external surroundings and more to their unfavorable, self-targeted cognitions when confronting a social-evaluative experience. Other studies have reported an information-processing bias for internal physiological cues quite than external social threat stimuli (Mansell et al. In a series of experimental studies, Bogels and Lamers (2002) discovered that focusing consideration on the self increases social anxiety whereas focusing consideration on the duty reduces social anxiety. Similarly socially phobic people advised that their pulse fee had increased whereas anticipating a social interplay skilled larger anxiety and more unfavorable beliefs throughout a threatening social encounter (Wells & Papageorgiou, 2001; see Bogels et al. Another body of research has investigated how people evaluate their social performances and the way these evaluations evaluate to their actual stage of performance as decided by observers. In various studies people with social phobia rated their very own public performance on a social evaluative task. In their evaluate Heimberg and Becker (2002) concluded that people with social phobia do exhibit performance defcits in social evaluative situations however they also evaluate their performance much more negatively than others. We can conclude that research help for Hypothesis four is strong, with social phobia characterised by an internal attentional bias and exaggerated unfavorable interpretation of interoceptive cues indicative of hysteria, loss of control, and inadequate public performance. Hypothesis 5 Feared social situations will provoke within the socially phobic particular person maladaptive compensatory and security responses aimed at minimizing or suppressing the expression of hysteria. Alden and Bieling (1998) discovered that when socially anxious people used security behaviors throughout a regular dialog. In a more recent research people with social phobia reported larger use of security behaviors and exhibited bigger performance defcits in commonplace dialog and speech tasks than people with other anxiety issues or nonclinical controls (Stangier et al. A subsequent path evaluation revealed that security behaviors partially mediated group variations in social performance. At this point, just a few studies have investigated the role of security behaviors in social phobia however these initial fndings suggest that maladaptive security seeking could play a role within the persistence of social anxiety. More research is needed, especially on the relation between involuntary inhibitory habits and production of security-seeking coping responses. Hypothesis 6 Postevent processing of social situations is characterised by an specific autobiographical reminiscence bias for previous unfavorable social experiences in these with social phobia. Unlike other issues in which anxiety declines or ceases after escape from a threatening state of affairs, people with social phobia will experience recurrence of hysteria as they recall previous social incidents that had been embarrassing and related to perceived unfavorable evaluation. Postevent processing involving repeated biased recall and rumination about previous threatening social occasions will improve anticipatory anxiety for future social situations by offering schema-congruent evidence of social threat and ineptitude. Researchers have only lately begun to examine the role of postevent processing in social phobia. In a research by Mellings and Alden (2000), excessive and low socially anxious students, who participated in a regular social interplay, had been assessed for rumination and recall of the interplay 1 day later. The highly anxious group reported signifcantly more rumination and there was a tendency for postevent rumination to predict recall of unfavorable self-associated information about the day past�s interplay with the laboratory accomplice (see additionally Kocovski & Rector, 2008). Abbott and Rapee (2004) discovered that socially phobic people engaged in signifcantly more unfavorable rumination a few 3-minute impromptu speech given 1 week earlier and this was associated to how negatively they appraised their speech performance. In another research, excessive socially anxious students tended to recall more unfavorable and shameful reminiscences when requested to recall a previous ambiguous social occasion (Field, Psychol, & Morgan, 2004; see additionally Morgan & Banerjee, 2008). In their evaluate Brozovich and Heimberg (2008) concluded that self-report, diary, and experimental studies point out that postevent processing is a distinguished cognitive course of that contributes to social anxiety by reinforcing unfavorable impressions of oneself. Moreover, autobiographical reminiscence recall bias for the unfavorable aspects of previous social occasions could also be a pivotal cognitive characteristic of postevent processing that accounts for its results on anxiety. This is completed by lowering unfavorable rumination about previous performance and encouraging a more optimistic reappraisal of previous social performance and its consequence. Even though just a few studies have investigated anticipatory processing in social phobia, the preliminary fndings are supportive of the cognitive model. Mellings and Alden (2000) discovered that only a excessive social anxiety group turned more apprehensive about collaborating in a second commonplace social interplay 1 day after finishing an initial unstructured 10-minute dialog with a accomplice. Based on a semistructured interview that assessed intervals of anticipation before social interactions, Hinrichsen and Clark (2003) reported that the excessive socially anxious group (1) recalled more previous perceived social failures; (2) had been more conscious of unfavorable bodily sensations, thoughts and images; and (3) relied more on problematic cognitive strategies to handle their anticipatory anxiety. In a subsequent research both excessive and low socially anxious students who got anticipatory anxiety in comparison with distraction directions throughout 20 minutes of preparation for a speech exhibited signifcantly higher anxiety ratings (Hinrichsen & Clark, 2003; see additionally Vassilopoulos, 2008). Cognitive evaluation anD Case formulation Various critical reviews have been revealed on the cognitive and symptom measures specifcally developed for social anxiety. In this section we concentrate on a number of of the more frequent symptom measures in addition to a few specifc questionnaires that assess the cognitive profle of social phobia. We start with a quick consideration of standardized instruments for social phobia and finish with a framework for case formulation derived from the current model. Social phobics score signifcantly higher than other anxiety dysfunction groups or nonclinical controls. The questionnaire includes a thirteen-merchandise Agoraphobia subscale that was included to provide a greater differentiation of social phobia from agoraphobia (Beidel & Turner, 2007). In addition people with generalized social phobia score signifcantly higher than these with the circumscribed subtype (Ries et al. However, cutoff scores should be used cautiously and for screening only since 10% of nonclinical people score above the cutoff (Gillis, Haaga, & Ford, 1995). The 30-merchandise true/false scale was initially developed by Watson and Friend (1969) to assess expectation, apprehension, distress, and avoidance of social evaluative situations. Moreover, it has optimistic correlations with other measures of social anxiety and people with social phobia score signifcantly higher than these with panic dysfunction or a community pattern (Collins, Westra, Dozois, & Stewart, 2005). However, confrmatory issue evaluation revealed issues with the four reverse-scored objects (Duke, Krishnan, Faith, & Storch, 2006; Rodebaugh, Woods, et al. Some researchers have eliminated the role play and instruct people to fee frequency of thoughts before, throughout, or after any interactions with the opposite intercourse (Dodge, Hope, Heimberg, & Becker, 1988). It has excessive check�retest reliability and signifcantly differentiates social phobia from other anxiety issues. The measure correlates with other cognition and signs measures of social anxiety and is sensitive to remedy results. Case Conceptualization A cognitive case formulation explicates the key cognitive and behavioral processes responsible for heightened anxiety in the course of the anticipatory, exposure, and postevent processing phases of social phobia. The case formulation follows the overall format we outlined in Chapter 5 with specific application to the unique cognitive processes proposed within the cognitive model of social phobia (see Figure 9. Situational Analysis the cognitive therapist begins by identifying the total vary of social situations that the client fnds anxiety-scary and may keep away from. It is necessary to identify mildly anxious situations in addition to people who elicit intense anxiety and avoidance. Furthermore, self-monitoring varieties just like the Situational Analysis Form (Appendix 5. Determine relative �� How usually are anticipatory anxiety, exposure, and postevent processing contribution of the three related to each concern social situationfl Assess for specific threat �� What is the character of the perceived threat related to each concern interpretation bias situationfl Assess heightened �� What is the extent of excessive self-consciousness and self-targeted self-targeted consideration, awareness in social situationsfl
Nihilistic delusions involve the conviction that a major disaster will happen 12.5mg esidrix with visa, and somatic delusions focus on preoccupations concerning health and organ function purchase 12.5 mg esidrix overnight delivery. An ex� ample of a nonbizarre delusion is the assumption that one is under surveillance by the police cheap esidrix 12.5mg mastercard, de� spite an absence of convincing evidence buy esidrix 25mg free shipping. The distinction between a de� lusion and a strongly held thought is usually difficult to make and relies upon partly on the degree of conviction with which the assumption is held regardless of clear or reasonable contradictory evidence concerning its veracity. Hallucinations Hallucinations are notion-like experiences that happen with out an exterior stimulus. They are vivid and clear, with the total drive and impact of normal perceptions, and never under voluntary management. They could happen in any sensory modality, but auditory halluci� nations are the commonest in schizophrenia and related problems. The hallucinations should happen within the con� text of a clear sensorium; those who happen whereas falling asleep (hypnagogic) or waking up (hypnopompic) are considered to be inside the range of normal experience. Hallucinations may be a standard a part of spiritual experience in sure cultural contexts. The particular person could swap from one subject to another derailment or loose associa� tions). Answers to questions may be obliquely related or fully unrelated (tangentiality). Because mildly disorganized speech is widespread and nonspecific, the symptom have to be se� vere sufficient to substantially impair effective communication. The severity of the impair� ment may be difficult to evaluate if the person making the prognosis comes from a different linguistic background than that of the person being examined. Less extreme dis� organized thinking or speech could happen in the course of the prodromal and residual intervals of schizophrenia. Grossly Disorganized or Abnormai iViotor Behavior (inciuding Catatonia) Grossly disorganized or abnormal motor conduct could manifest itself in quite a lot of methods, starting from childlike "silliness" to unpredictable agitation. Problems may be famous in any type of aim-directed conduct, resulting in difficulties in performing actions of every day dwelling. This ranges from resistance to directions negativism); to maintaining a rigid, inappropriate or bi� zarre posture; to a complete lack of verbal and motor responses mutism and stupor). It can also embrace purposeless and extreme motor exercise with out obvious trigger pleasure). Other options are repeated stereotyped actions, staring, grimacing, mutism, and the echoing of speech. Although catatonia has historically been associated with schizophrenia, catatonic signs are nonspecific and will happen in different psychological problems. Negative Symptoms Negative signs account for a considerable portion of the morbidity associated with schizophrenia but are much less prominent in different psychotic problems. Two unfavorable symp� toms are particularly prominent in schizophrenia: diminished emotional expression and avolition. Diminished emotional expression consists of reductions within the expression of emo� tions within the face, eye contact, intonation of speech (prosody), and actions of the hand, head, and face that usually give an emotional emphasis to speech. The particular person could sit for long intervals of time and present little interest in taking part in work or social actions. Anhedonia is the decreased capacity to experience pleasure from constructive stimuli or a degradation within the recollection of pleasure previously experienced. Asociality refers to the apparent lack of interest in social interactions and may be associated with avo� lition, however it can also be a manifestation of limited opportunities for social interactions. Finally, the prognosis of a schizophrenia spectrum disorder requires the exclusion of another con� dition that may give rise to psychosis. Abnormalities of beliefs, thinking, and notion are beneath the threshold for the diagno� sis of a psychotic disorder. Two situations are defined by abnormalities limited to one area of psychosis: delu� sions or catatonia. Delusional disorder is characterised by at least 1 month of delusions but no different psychotic signs. Schizophreni� type disorder is characterised by a symptomatic presentation equal to that of schizo� phrenia except for its period (less than 6 months) and the absence of a requirement for a decline in functioning. Schizophrenia lasts for at least 6 months and consists of at least 1 month of active-section signs. In schizoaffective disorder, a temper episode and the active-section signs of schizophrenia happen together and were preceded or are followed by at least 2 weeks of de� lusions or hallucinations with out prominent temper signs. In substance/medicationinduced psychotic disorder, the psychotic signs are judged to be a physiological con� sequence of a drug of abuse, a medicine, or toxin exposure and stop after elimination of the agent. In psychotic disorder due to another medical condition, the psychotic signs are judged to be a direct physiological consequence of another medical condition. Catatonia can happen in several problems, together with neurodevelopmental, psychotic, bi� polar, depressive, and different psychological problems. This chapter also consists of the diagnoses catatonia associated with another psychological disorder (catatonia specifier), catatonic disorder due to another medical condition, and unspecified catatonia, and the diagnostic standards for all three situations are described together. Clinician-Rated Assessment of Symptoms and Related Clinical Phenomena in Psychosis Psychotic problems are heterogeneous, and the severity of signs can predict impor� tant aspects of the illness, such because the degree of cognitive or neurobiological deficits. The severity of temper signs in psychosis has prognostic worth and guides therapy. Thus, dimensional assessments of depres� sion and mania for all psychotic problems alert clinicians to temper pathology and the necessity to treat the place applicable. Many people with psychotic problems have impairments in a variety of cognitive domains that predict useful status. Clinical neuropsychological as� sessment can help guide prognosis and therapy, but transient assessments with out formal neuropsychological assessment can provide useful information that may be enough for diagnostic purposes. Formal neuropsychological testing, when carried out, must be advert� ministered and scored by personnel skilled in the usage of testing devices. Schizotypal (Personality) Disorder Criteria and text for schizotypal personality disorder may be discovered within the chapter "Person� ality Disorders. If manic or main depressive episodes have occurred, these have been transient relative to the period of the delusional intervals. Specify whether: Erotomanie type: this subtype applies when the central theme of the delusion is that another person is in love with the person. Grandiose type: this subtype applies when the central theme of the delusion is the conviction of having some great (but unrecognized) talent or insight or having made some important discovery. Jeaious type: this subtype applies when the central theme of the person�s delusion is that his or her partner or lover is untrue. Persecutory type: this subtype applies when the central theme of the delusion in� volves the person�s perception that she or he is being conspired towards, cheated, spied on, followed, poisoned or drugged, maliciously maligned, harassed, or obstructed within the pursuit of long-time period objectives. Somatic type: this subtype applies when the central theme of the delusion entails bodily capabilities or sensations. Specify if: the following course specifiers are only to be used after a 1-yr period of the disorder: First episode, presently in acute episode: First manifestation of the disorder meet� ing the defining diagnostic symptom and time standards. First episode, presently in partial remission: Partial remission is a time period dur� ing which an improvement after a previous episode is maintained and in which the de� fining standards of the disorder are only partially fulfilled. Subtypes In erotomanie type, the central theme of the delusion is that another person is in love with the person. In grandiose type, the central theme of the de� lusion is the conviction of having some great talent or insight or of having made some im� portant discovery. Less generally, the person could have the delusion of having a particular relationship with a prominent particular person or of being a prominent person (in which case the precise particular person may be regarded as an impostor). In jealous type, the central theme of the delusion is that of an un� trustworthy partner. This perception is arrived at with out due trigger and is predicated on incorrect infer� ences supported by small bits of "evidence". The particular person with the delusion often confronts the partner or lover and attempts to intervene within the imagined infidelity. The affected particular person could engage in repeated attempts to obtain satisfaction by legal or legislative action. Indi� viduals with persecutory delusions are often resentful and offended and will resort to vio� lence towards these they imagine are hurting them. In somatic type, the central theme of the delusion entails bodily capabilities or sensations. Diagnostic Features the important function of delusional disorder is the presence of one or more delusions that persist for at least 1 month (Criterion A). If temper episodes happen concurrently with the delusions, the total period of these temper episodes is transient relative to the total period of the delusional intervals (Criterion D). Associated Features Supporting Diagnosis Social, marital, or work issues may result from the delusional beliefs of delusional dis� order. Individuals with delusional disorder might be able to factually describe that others view their beliefs as irrational but are unable to settle for this themselves. Many people develop irritable or dysphoric temper, which may often be understood as a reaction to their delusional beliefs. Anger and violent conduct can happen with persecutory, jealous, and erotomanie types. Prevaience the lifetime prevalence of delusional disorder has been estimated at round zero. Deveiopment and Course On average, international function is generally better than that observed in schizophrenia. Al� although the prognosis is generally stable, a proportion of people go on to develop schizophrenia. Delusional disorder has a significant familial relationship with both schizophrenia and schizotypal personality disorder. Although it could possibly happen in younger age groups, the condition may be extra prevalent in older people. Functional Consequences of Delusional Disorder the useful impairment is often extra circumscribed than that seen with different psy� chotic problems, though in some circumstances, the impairment may be substantial and embrace poor occupational functioning and social isolation. When poor psychosocial functioning is present, delusional beliefs themselves typically play a significant function. If a person with obsessive-compul� sive disorder is completely satisfied that his or her obsessive-compulsive disorder beliefs are true, then the prognosis of obsessive-compulsive disorder, with absent insight/delu� sional beliefs specifier, must be given rather than a prognosis of delusional disorder. Similarly, if a person with body dysmorphic disorder is completely satisfied that his or her body dysmorphic disorder beliefs are true, then the prognosis of body dysmor� phic disorder, with absent insight/delusional beliefs specifier, must be given rather than a prognosis of delusional disorder. Delirium, main neurocognitive disorder, psychotic disorder due to another medical con� dition, and substance/medicine-induced psychotic disorder. Individuals with these problems could present with signs that recommend delusional disorder. For example, sim� ple persecutory delusions within the context of main neurocognitive disorder can be di� agnosed as main neurocognitive disorder, with behavioral disturbance. A substance/ medicine-induced psychotic disorder cross-sectionally may be similar in symptom� atology to delusional disorder but may be distinguished by the chronological relationship of substance use to the onset and remission of the delusional beliefs. Delusional disorder may be distinguished from schizophrenia and schizophreniform disorder by the absence of the other character� istic signs of the active section of schizophrenia. These problems may be distinguished from delusional disorder by the temporal relationship between the temper disturbance and the delusions and by the severity of the temper signs. If delusions oc� cur solely during temper episodes, the prognosis is depressive or bipolar disorder with psychotic options.
Order esidrix in united states online. Are medicines for thyroid lifelong??.
![]()
spla.pro is already a rich, multilingual database that lists nearly artists, cultural events, professional organizations, 3 500 venues, films, books, albums, shows, etc.
spla.pro also provides comprehensive listings for some 700 ACP country festivals and benefits from the reputation and media impact of Africultures (750 000 visits a month on africultures.com, plus a weekly newsletter sent to over 180 000 subscribers) and africinfo.org (a weekly African cultural events newsletter) run by the Groupe 30-Afrique.



















Add your information (With the self-presentation files)
Convention with Wikiafrica / Wikipedia : Southplanet's contents are shared for free according to the licence Creative commons  .
.
© Some artistic content (photos, videos, sound recordings, written texts) is subject to copyright. Copyright is mentioned when and where it applies. Copyrighted material cannot be reproduced.
